

Introduction:
Cryopreserved peripheral blood stem cell (PBSC) products are thawed at bedside and infused by gravity through a large bore central venous line (CVL). Peripherally inserted central venous catheters (PICC) are routinely used for infusion of blood products and medications but are rarely used to administer hematopoietic progenitor cells (HPC). The rationale for this practice is not well established but the general assumption is that the smaller gauge sizes of the PICC and resultant decreased infusion rates would damage the HPCs. The use of PICC to infuse HPCs can have many benefits, such as patient comfort, cost effectiveness, and reducing potential line-related complications from the insertion of a large bore, and often additional, CVL. These line-related complications include infections, pneumothorax, haematomas, etc. The aim of this prospective observational study is to present the experience of using PICC in lymphoma patients receiving autologous PBSC transplantation in terms of the safety and efficacy.
Methodology:
From September 2019 to June 2020, a prospective observational study involving 16 patients with lymphoma undergoing autologous PBSC transplantation was conducted in National University Cancer Institute, Singapore (NCIS). The patients were divided into 2 groups - the first group included 9 lymphoma patients who received their autologous PBSC transplant via PICC, while the second/control group included 7 lymphoma patients who received the treatment via a large bore CVL. The types of PICC and CVL inserted for the patients were standardized - 19G dual lumen PICC and 7Fr triple lumen non-tunnelled CVL respectively. All the CVLs were inserted in the right internal jugular vein, while the PICC were inserted in either the brachial or basilic veins. All patients in both groups underwent BEAM conditioning transplantation regime prior to autologous PBSC transplantation. The duration of the catheter-in-situ, catheter-associated complications, PBSC infusion rate, CD34 cell dose, total nucleated cell dose infused, and the time for absolute neutrophil and platelet count engraftment were analysed for the study.
Results:
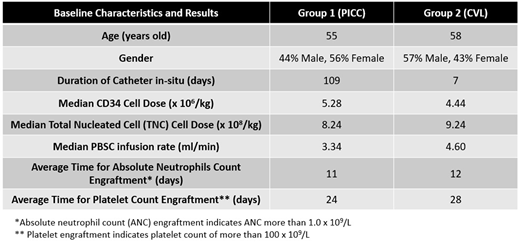
The baseline characteristics and results for both groups are shown in Table 1.
It is important to highlight that for the first group using PICC, none of them had any adverse event from PBSC transplantation. 44.4% of the patients had only minor issues during the PBSC infusion, mainly due to slower infusion rate and sediments were seen in the tubing of the PICC. These issues were quickly overcome by manual flushing of the PICC with normal saline fluid boluses. Only 1 out of 9 had a mild skin irritation at the insertion site of the PICC. For the second/control group using CVL, 43% of them had both PICC and CVL in-situ at one point of their treatment. These patients underwent an additional procedure for CVL insertion and the CVL was removed within 2 weeks of insertion. Only 1 out of 7 patients had minor issue of severe nausea during the PBSC infusion. There was no adverse event during the PBSC infusion or catheter associated complication.
Conclusion:
Our study showed that the use of PICC is safe and effective for patients receiving autologous PBSC transplantation, compared to the conventional large bore central venous catheters. Despite having longer PBSC infusion rate for PICC, the time taken for neutrophil and platelet recovery between both groups were comparable and there were no serious complications.
Chng:Celgene: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Amgen: Honoraria, Research Funding; Abbvie: Honoraria; Novartis: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal